Abstract
Pectus Carniatum (PC) is a term used to describe a range of different chest wall deformities characterized by anterior protrusion of sternum and attached ribs. Depends on involvement of the components of sternum, it is divided into chondrogladiolar and chondromanubrial. It is the second most common chest deformity observed in children. The exact pathogenesis of PC is not cleared. It seems that it is as a result of abnormal costal cartilage growth. It may be associated with scoliosis (15%), congenital heart disease, Marfan syndrome and other connective tissue disorders.
Keywords
Bracing, Pectus Carniatum
Introduction
Pectus Carniatum (PC) is a term used to describe a range of different chest wall deformities characterized by anterior protrusion of sternum and attached ribs [1,2]. Depends on involvement of the components of sternum, it is divided into chondrogladiolar and chondromanubrial. It is the second most common chest deformity observed in children [3]. The exact pathogenesis of PC is not cleared. It seems that it is as a result of abnormal costal cartilage growth. It may be associated with scoliosis (15%), congenital heart disease, Marfan syndrome and other connective tissue disorders [2].
Most of the subjects live with PC without special symptoms or signs. The main problem of these subjects is cosmetic problem as the deformity stand out in speat of wearing cloths [4]. Use of conservative treatment and surgery are the two most common treatment approaches used for the subjects with PC [1,5]. Bracing is one of the conservative treatments used for the subjects with PC. Evidences support the use of brace return to 1977 [3,6]. Haje and Bowen published their bracing experience in 1992. However, strong evidences on use of this brace published by Canadian pediatric surgeons [1,2,7,8].
The bracing protocol is based on application of long term continues pressure at the deformity protrusion to allow costal cartilage remodeling [9]. The available braces for PC surrounding the thorax and apply pressure on anterior and posterior parts of spine [1,3,6]. There are some evidences on use of braces on PC deformities. However, it is controversial how effective is use of brace in treatment of PC deformity. Therefore, the aim of this review was to determine the efficiency of available braces and also to determine the time and duration of brace usage to have maximum efficiency.
Method
A search was done in some data bases including Google Scholar, PubMed, ISI web of Knowledge, Cochrane centered register of controlled trial (CCTR), Cochrane data bases of systematic reviews (CDSR), data bases of abstracts of reviews effects (DARE) and Embase. Some key words such as Pectus Carniatum, Pigeon chest were used in combination with brace, orthosis, and conservative treatment.
The first eligibility criteria for selection of studies were based on population (only studies on Pectus Carniatum were selected) and linguistic range (only studies reported in English were included). It should be emphasized that the nature of studies and outcome variables were not considered in the selection of the studies.
Type of studies: Although the emphasis of this study was to focus mostly on randomized control trials, due to lack of these studies on this topic other types of studies were also included. Some low evidence such as abstracts, conference articles, editorial comments, and expert opinion were excluded from the final list.
Type of participants: The studies focus on the subjects with PC were selected in this study.
Type of interventions: The studies on use of brace or orthosis were selected in this study. The studies focused on surgery or on comparison between surgery and conservative treatment were excluded from the review.
Type of outcomes: The main outcome measures selected in this study included: X-Ray measures (asymmetry index, angle of sternal rotation), time of follow up, and satisfaction degree.
Secondary outcome: The need for surgery and other complications were selected as secondary outcomes.
Selection of the studies: Two researchers independently screened the studies based on the aforementioned criteria. It was done mostly based on titles and abstracts.
Data extraction and management: This review was done based on PICO (population, intervention, comparison and outcomes) style. It means that the data of each study was categorized as population, intervention, comparison, and outcomes.
Quality assessment and determination of the risk of bias: The quality of the studies was evaluated based on Down and Black tool. It is a reliable tool to evaluate the quality of the studies. Figure 1 shows the procedure selected in this study.
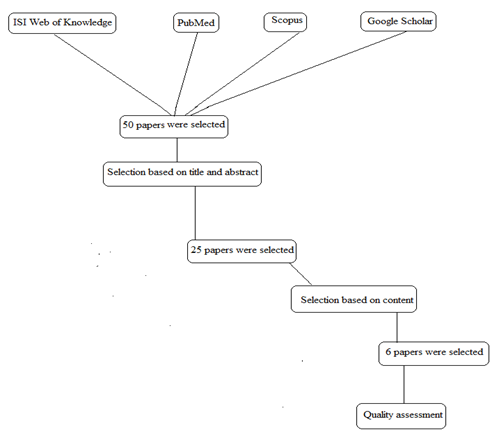
Figure 1. The procedure used in this review to select the studies.
Results
There were 25 studies on use of braces on Pectus Carniatum (PC). Based on titles and abstracts 15 papers were selected. Finally, 6 papers were selected for final analysis. The quality of the studies based on Down and Black tool checklist varied between 4 and 18. The results of the available studies confirmed the following points:
- No specific complications associated with use of brace except initial discomfort when wearing the brace.
- Compressive orthosis is a successful method of PC treatment
- Patient’s satisfaction, posture and QLF were better in the subject’s received bracing and physical therapy.
Discussion
Pectus Carniatum (PC) is one of the deformities of chest wall with high incidence amongst the other chest deformities. Use of braces is the main treatment approaches used for the subjects with PC [9]. The aim of this review was to determine the efficiency of bracing on correction of this deformity.
There were 6 papers on this topic with quality varied between 4 and 18. The quality of the available studies was low due to small number of the subjects participated in the studies, and no attempt was done to blind the researchers and participants from interventions.
The main question posted here is that weather this kind of treatment approach is effective in correction of PC deformity or not. There were 6 studies which evaluated the efficiency of bracing on PC. Various parameters have been used to determine the efficiency of this treatment approach. In the research done by Lee et al., 119 patients treated with brace followed for a period of 2 to 3 months [6]. The results of this study showed that no special complications were associated with use of bracing. Subjects confirmed that they had only discomfort when wearing the brace and also some skin rush [6].
Asymmetry index and angle of sternal rotation were the parameters evaluated in the study of Stephenson and Bois after brace treatment. The results of this study showed that 24 subjects reported good or excellent results, however 8 subjects required surgery. They also confirmed that compressive bracing is a successful method for PC treatment [10]. Alaca et al. showed that posture, quality of life and treatment satisfaction scores were better in those treated with brace and exercise [11]. It seems that pulmonary function did not influence by bracing. However, angle of rotation of sternum and patients’ satisfaction increased significantly.
Long term monitoring of output of treatment with brace was done by Mielke and Wniter. They showed that after 7 years of treatment excellent results without recurrent deformity was achieved [12]. In other available studies, it was shown that pulmonary function was not affected by bracing [13]. Moreover, compressive orthosis is a safe and effective alternative to surgical repair for this deformity [7]. Based on the results of above mentioned studies and due to number of the subjects participated in each study and follow up duration it can be concluded that use of compressive bracing is an effective treatment approach to correct PC deformity. It seems that there is no important side effects associated with this treatment approach. Therefore, this method is recommended to be used for those with PC deformity.
There are some limitations associated with available studies. The main limitation is that the efficiency of bracing on PC deformity was only evaluated based on QOL, symmetry, and satisfaction of the patients. There is no study which evaluated the efficiency of treatment based on all of mentioned parameters and in a large number of the subjects. Therefore, it is recommended that the efficiency of bracing will be evaluated in big number of the subjects with PC deformity and after a long period of follow up.
|
Reference |
Method |
Results |
|
Lee et al. [6] |
Participants: 119 patients Age: 12.9 ± 4.3 Intervention: Bracing Comparison: satisfaction degree Follow up: 2 to 3 months |
Average satisfaction: 3.95 ± 0.4 No special complication occurred in use of brace. Only small discomfort was seen when wearing the brace (skin rush=70.6%, skin discomfort=15.1%) |
|
Stephenson et al. [10] |
Participants: 63 patients Age: 7 to 18 (13.3 ± 2.5) Intervention: 17 patients with mild defects elected observation and 46 begun bracing protocol. Comparison: Asymmetry index, angle of sternal rotation |
Finally, 36 subjects were selected. 8 failed bracing because of noncompliance. 24 subjects reported both good or excellent results and 8 subjects required surgery. It seems that compressive orthosis is a successful method for PC treatment. |
|
Alaca et al. [11] |
Participants: 30 patients with PC deformity were divided into two groups, brace group and brace and exercise group. Age: 13.66 ± 1.46 and 13.9 ± 1.44, respectively. Intervention: bracing and bracing and exercise Comparison: QOL, patient’s perception of deformity and treatment satisfaction. |
Patient’s perception of deformity, posture, QOL, and treatment satisfaction scores were better in group 2. |
|
Ates et al. [13] |
Participants: 53 patients with PC deformity. Intervention: Orthotic treatment Comparison: Pulmonary function (spirometry), Pectus severity index, angle of sternal rotation. |
Pulmonary function was not affected by bracing. Angle of rotation increased by 47%. Overall satisfaction was 3.92 ± 0.27. |
|
Mielke and Wniter [12] |
Participant: A 14 years old girl. Intervention: corrective underarm for 6 months and then full time bracing for 7 months. |
After 7 years of treatment, excellent results without recurrent of deformity was achieved. |
|
Banever et al. [7] |
Participants: 24 subjects with PC deformity. Age: 3-16 years. Intervention: Brace Follow up: 3 months Comparison: correction of the deformity, complications. |
5 subjects had little or no improvement. 15 subjects had significant to complete correction. No complication associated with this study. It seems that compressive orthosis is a safe and effective alternative to surgical repair in this deformity. |
|
Reference |
Reporting |
External validity |
Internal validity-bias |
Internal validity-selection bias |
Power |
|
[10] |
9 |
2 |
3 |
3 |
1 |
|
[6] |
8 |
2 |
2 |
2 |
1 |
|
[11] |
9 |
2 |
5 |
2 |
1 |
|
[7] |
6 |
1 |
2 |
1 |
0 |
|
[13] |
7 |
1 |
3 |
1 |
0 |
|
[12] |
4 |
0 |
0 |
0 |
0 |
Conclusion
Based on the available studies it can be concluded that compression bracing is an effective treatment approach which can be used for the subjects with PC. There is no study in literature evaluated the efficiency of this approach based on severity of the disease, duration of use, and age of the subjects. Therefore, it is recommended that the effects of the mentioned parameters will be evaluated in a study with big number of the participants.
References
2. McHam B, Winkler L. Pectus Carinatum. In: StatPearls. StatPearls Publishing LLC.: Treasure Island (FL). 2021.
3. Hunt I, Patel AJ. Effectiveness of Compressive External Bracing in Patients with Flexible Pectus Carinatum Deformity: A Review. Thorac Cardiovasc Surg. 2020;68(1):72-79.
4. Rimessi A, Mazzucco A, Fieschi S, Torre M. Therapeutical options in pectus carinatum in young patients. Pediatric Medicine. 2019;2: 17-17.
5. Haje SA, de Podestá Haje D. Orthopedic approach to pectus deformities: 32 years of studies. Revista Brasileira de Ortopedia (English Edition). 2009 Jan 1;44(3):191-8.
6. Lee SY, Lee SJ, Jeon CW, Lee CS, Lee KR. Effect of the compressive brace in pectus carinatum. European journal of cardio-thoracic surgery. 2008 Jul 1;34(1):146-9.
7. Banever GT, Konefal Jr SH, Gettens K, Moriarty KP. Nonoperative correction of pectus carinatum with orthotic bracing. Journal of Laparoendoscopic & Advanced Surgical Techniques. 2006 Apr 1;16(2):164-7.
8. Emil S. Current options for the treatment of pectus carinatum: When to brace and when to operate?. European Journal of Pediatric Surgery. 2018 Aug;28(04):347-54.
9. Burjonrappa S, Sosulski AB, Hsieh L. A Review of Current Treatment Trends in Pediatric Chest Wall Abnormalities. J Pediatr Neonatal Care. 2017;6(1):00231.
10. Stephenson JT, Du Bois J. Compressive orthotic bracing in the treatment of pectus carinatum: the use of radiographic markers to predict success. Journal of Pediatric Surgery. 2008 Oct 1;43(10):1776-80.
11. Alaca N, Alaca İ, Yüksel M. Does physiotherapy applied in conjunction with compression brace treatment in patients with pectus carinatum have efficacy? A preliminary randomized-controlled study. Pediatric Surgery International. 2020 Jul;36:789-97.
12. Mielke CH, Winter RB. Pectus carinatum successfully treated with bracing: a case report. International Orthopaedics. 1993 Dec;17:350-2.
13. Ateş O, Karakuş OZ, Hakgüder G, Olguner M, Akgür FM. Pectus carinatum: the effects of orthotic bracing on pulmonary function and gradual compression on patient compliance. European Journal of Cardio-Thoracic Surgery. 2013 Sep 1;44(3):e228-32.